








































Hospital on wheels treats stroke victims in the field
UCLA and the Los Angeles County Fire Department are using a Mobile Stroke Unit to treat stroke victims in the field, saving them brain cells and possibly their life
A specialized ambulance could one day save your life from a stroke in the driveway of your home or a public parking lot. Everything needed to diagnose and treat the stroke fits inside, bringing the hospital to the patient.
That’s a reality in a select group of cities around the country. Right now, University of California, Los Angeles and the Los Angeles County Fire Department are collaborating to operate a Mobile Stroke Unit (MSU). The unit is being used in a national study to test the cost effectiveness and long-term patient outcomes of faster treatment.
“It’s been like night and day,” said Kenny Harrell, a firefighter and paramedic with the LA county fire department. As part of his job, Harrell operates both a standard ambulance, and drives the Mobile Stroke Unit.
Every minute a stroke victim is untreated, they lose two million brain cells. Time spent driving back to the hospital could lead to lifelong, debilitating side effects.
“One may become paralyzed on one side of their body, unable to speak or understand, or unable to walk,” said Dr. May Nour, medical director of the UCLA Mobile Stroke Program.
The stroke unit on wheels is staffed with a neurologist, nurse, CT technician and a paramedic. Doctors can video conference in and look at the patient using a high-resolution, 270-degree camera.

The stroke unit on wheels is staffed with a neurologist, nurse, CT technician and a paramedic. Doctors can video conference in and look at the patient using a high-resolution, 270-degree camera. Here is a video conferencing unit that doctors use. (Fox News)
Paramedics put the patient inside the unit the same way they’d load a patient into an ambulance. The nurse and technicians take over from there to determine what type of stroke the patient is having and administer treatment.
“One stop shop. We can do labs, we can do CT scan, physician evaluation and we can give the medications,” said Nour. “We don’t wait for transport time. We don’t wait for the patient to get to the hospital. We get to them and treat them in the most expedient way possible.”
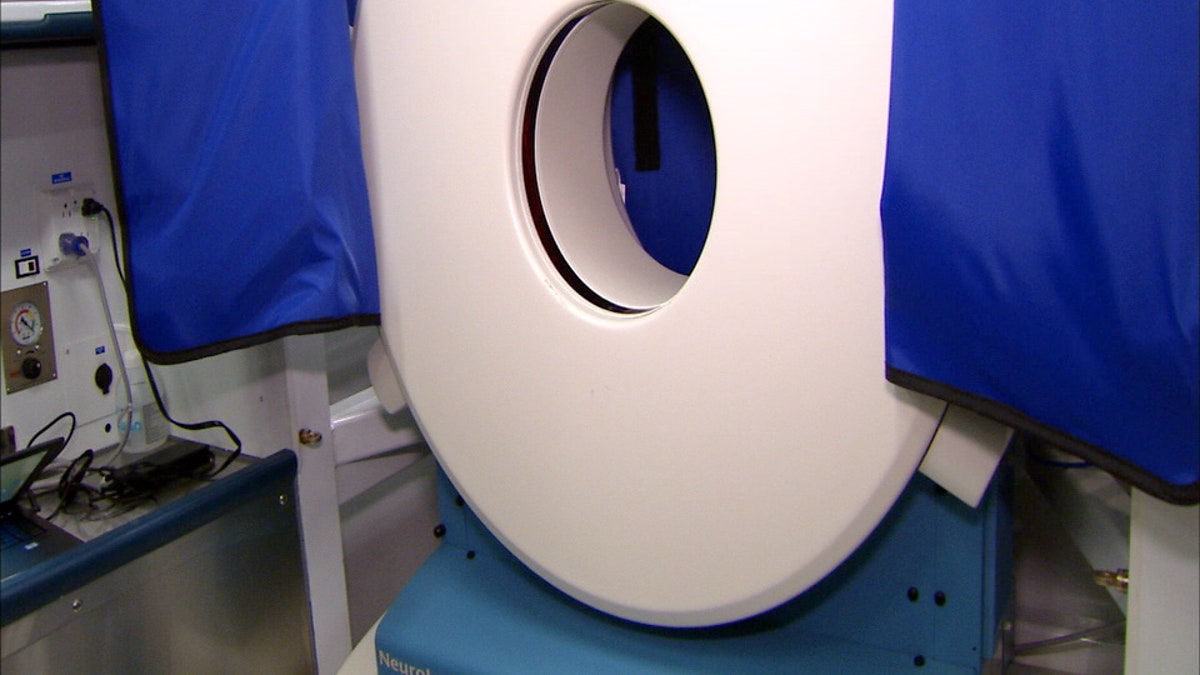
“One stop shop. We can do labs, we can do CT scan, physician evaluation and we can give the medications,” said Dr. May Nour, medical director of the UCLA Mobile Stroke Program. “We don’t wait for transport time. We don’t wait for the patient to get to the hospital. We get to them and treat them in the most expedient way possible.” Here is a CT scanner used to determine the type of stroke the patient is having. (Fox News)
Doctors say the MSU may be especially helpful in very rural and heavy traffic urban areas. In small towns, some stroke patients could live a half hour away from the nearest hospital, while in big cities like Los Angeles, traffic can triple the time of a ride that’s just a few miles away.
Eliminating the time it takes to drive back to the hospital could save tens of millions of brain cells, which could be the difference between surviving, walking, talking or even death.
“If I have a stroke that affected my right hand, which is my dominate hand, I can’t do my job anymore. Which is something, it’s part of my identity. Being a physician is not just what I do, it’s who I am,” Dr. Clayton Kazan, Medical Director of the Los Angeles County Fire Department.
If a patient becomes disabled as a result of the stroke, the costs could be lifelong.
“What are the direct and indirect medical costs as a result of somebody who’s unable to care for themselves, unable to participate in the work field, the health insurance costs for the rest of that person’s life,” Nour said.
Estimates for other stroke units across the country put the cost between $500,000 and $1,000,000. There are also staffing costs for the nurses, technicians and paramedics. Currently, those costs are mostly funded by private donations, with taxpayers sharing some of the staffing costs. But if use of these units continued, they'd be paid for by taxpayer dollars, and insurance providers, prompting more research about whether those costs would be sustainable.
Doctors believe even if the cost is high, Mobile Stroke Units are justified. There’s still a long way to go, however, before Mobile Stroke Units become standard across the country, if they ever do.
“If this unit does prove to be successful and patient outcomes are improved by its response,” Kazan said. “We have a lot of questions still to answer about how we would actually scale it up into a system as big as ours that actually has about 10 million people.”